The digital transformation of healthcare is failing, and skills are the reason.
Healthcare organizations have invested hundreds of billions in digital infrastructure. Yet 49% of healthcare CEOs report that their digital transformation investments have not delivered the expected benefits. Only 14% of healthcare workers report advanced digital skills. Three-quarters lack proficiency with generative AI. Even among Gen Z healthcare workers, 69% feel underprepared for digitally driven roles.
This white paper presents the evidence base, a segmented workforce typology, and the Wordsburg Digital Readiness Framework, a structured approach to closing the gap in ways that are clinically sensitive, operationally realistic, and measurably effective.

Key statistics: The scale of the healthcare digital skills crisis in 2026

Key Findings
| Theme | Finding | Stat | Source |
|---|---|---|---|
| Skills Gap | Healthcare workers with advanced digital skills | 14% | MRINetwork, 2026 |
| Skills Gap | Healthcare workers lacking generative AI proficiency | 75% | MRINetwork, 2026 |
| Skills Gap | Average time to fill AI roles in healthcare | 6 to 7 months | IDC, 2026 |
| Transformation Gap | Healthcare CEOs reporting digital transformation underdelivered | 49% | |
| Transformation Gap | EHR implementations failing to meet original objectives | 50 to 70% | |
| Transformation Gap | EHR implementations rated successful | 38% | KLAS, 2025 |
| Cost of Inaction | Projected global losses from AI skills gaps by 2026 | $5.5 trillion | IDC |
| Cost of Inaction | Potential annual healthcare savings from AI applications | $150 billion | Accenture |
Digital Readiness
A System Built for Yesterday, Staffed for the Day Before
Healthcare has never moved slowly in clinical innovation. Digital transformation is different. It restructures how information flows, how decisions are made, and how organizations are managed. That systemic nature is precisely what makes it so difficult to address through conventional training approaches.
A nurse learning a medication protocol masters one thing. A nurse learning to work within an AI-assisted clinical decision support system must understand data interpretation, flag false positives, maintain documentation discipline, and integrate digital outputs into human judgment, simultaneously, at clinical speed, without compromising patient safety.
Insufficient worker skills rank as the top obstacle to integrating AI into existing workflows, not technology limitations, budget constraints, or leadership scepticism.
IDC estimates that AI skills shortages alone may cost the global economy up to $5.5 trillion by 2026. In healthcare, AI roles take an average of six to seven months to fill, the longest of any sector measured. Among 94% of CEOs and CHROs who identify AI as their top in-demand skill, only 35% report having effectively prepared employees for AI-related roles.

Four Workforce Segments: Four Different Skills Crises
The digital skills gap is not monolithic. It presents differently in terms of severity, nature, and consequences across clinical, administrative, IT, and leadership segments. Effective intervention requires a segmented understanding before a unified response.

Four workforce segments, gap severity, and role-specific skill requirements. Wordsburg Healthcare Digital Readiness Analysis 2026.

What Underinvestment In Digital Readiness Actually Costs
The tendency in healthcare organizations is to treat digital skills development as a training budget item to be optimized, deferred, or addressed reactively. The cost calculus of that approach is deeply unfavourable when the full picture is examined.
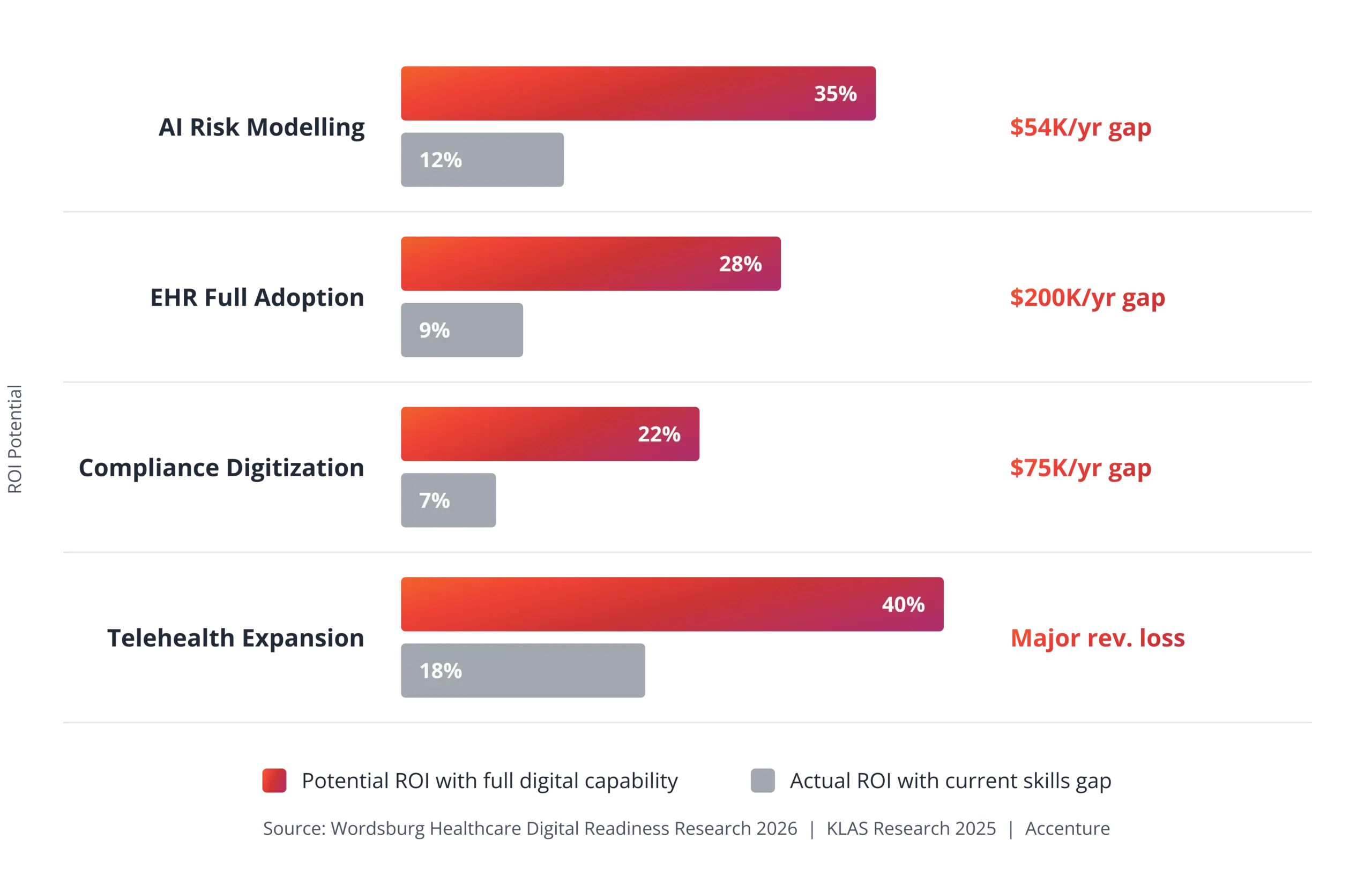
KLAS Research, 2025: Organizations that invest 15-20% of their implementation budget in training and change management are 2-3x more likely to meet project objectives. Among organizations that did not prioritize training, 57% of clinicians reported that their organizations did not adequately support implementation.

The Wordsburg Digital Readiness Framework
Closing the healthcare digital skills gap requires more than deploying e-Learning modules and hoping usage metrics improve. It requires a structured, phased program that begins with diagnostic rigor, accounts for the diversity of workforce personas, and builds capability progressively from awareness through to sustained, measurable practice change.
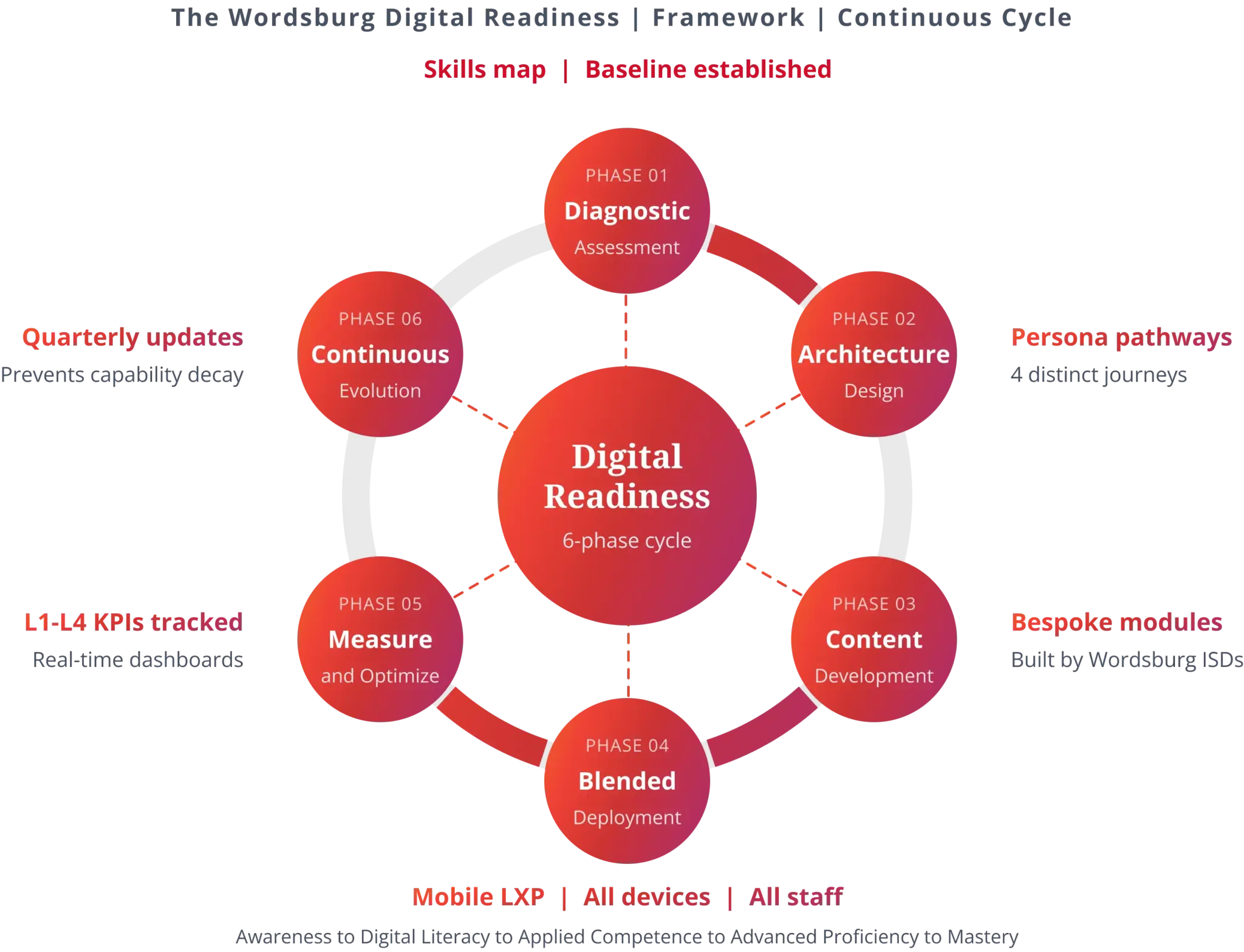
The Wordsburg Digital Readiness Framework: six phases, five competency levels, applied across all healthcare workforce segments
Phase 01: Diagnostic Assessment
The framework begins with a skills-mapping exercise using a Digital Competency Framework. This assessment identifies gaps by role, department, and risk, creating a baseline for measuring program outcomes. For organizations adopting new technology, the diagnostic should happen before, not after, deployment decisions.
Phase 02: Architecture Design
Learning pathways are tailored for clinical, administrative, IT, and leadership segments. Content, format, and delivery are matched to each audience’s needs. Programs that treat all roles identically yield poor results.
Phase 03: Content Development
Instructional designers create engaging, role-specific learning tied to real workflows. This includes EHR simulations, AI exercises, compliance scenarios, and leadership curricula, all customized to the customer’s context rather than relying on generic templates.
Phase 04: Blended Deployment
Training uses microlearning, simulation, virtual facilitation, and practice challenges delivered through mobile-optimized LMS and LXP platforms. Effective programs account for shift patterns, handovers, and the demands of clinical environments, rather than idealized conditions.
Contextual, bite-sized learning achieves higher engagement and retention than traditional e-Learning. VR simulations improve knowledge retention, and AI-personalized pathways deliver content tailored to each learner’s needs and timing.
Phase 05: Measurement & Optimization
Dashboards track progress from Awareness to Mastery at all levels, linking learning outcomes to operational metrics like productivity, errors, and system adoption. This connects training investment directly to business impact.
Phase 06: Continuous Evolution
Quarterly reviews ensure the program evolves with technology and regulations. Without ongoing updates, training quickly becomes outdated and risky.

What This Looks Like In Practice
The single greatest failure mode of digital skills programs in healthcare is designing for an ideal learner in an ideal setting. Healthcare professionals do not have uninterrupted blocks of time for training. They have clinical commitments, shift patterns, emergency demands, and emotional loads that make long-form eLearning modules a fantasy.
- Facilitated Leadership Workshops: Fortnightly 90-minute sessions for clinical and operational leaders and a digital fluency curriculum covering AI literacy, data interpretation, and change leadership
- Microlearning For Clinical Environments: 5–10-minute modules via mobile-optimized LXP, consumable during natural breaks in clinical workflows. Engagement rates reach 70-90%, compared with the 15-20% typical of longer formats
- Simulation-Based Practice: EHR workflow simulations and AI-output interpretation exercises in risk-free environments. VR-enabled simulations improve knowledge retention by 75% compared to passive content
- AI-Personalized Learning Pathways: LXP platforms that analyze individual performance and role context to generate adaptive pathways, so a clinical nurse and an administrative coordinator receive entirely different learning journeys from the same platform

From Training Metrics To Board-Level Outcomes
Healthcare learning and development has historically measured inputs: completion rates, hours trained, and modules accessed. These numbers are easy to produce and difficult to connect to anything a board or executive team cares about. Wordsburg’s measurement architecture is built on four Kirkpatrick levels, adapted for the specific operational context of healthcare digital transformation.
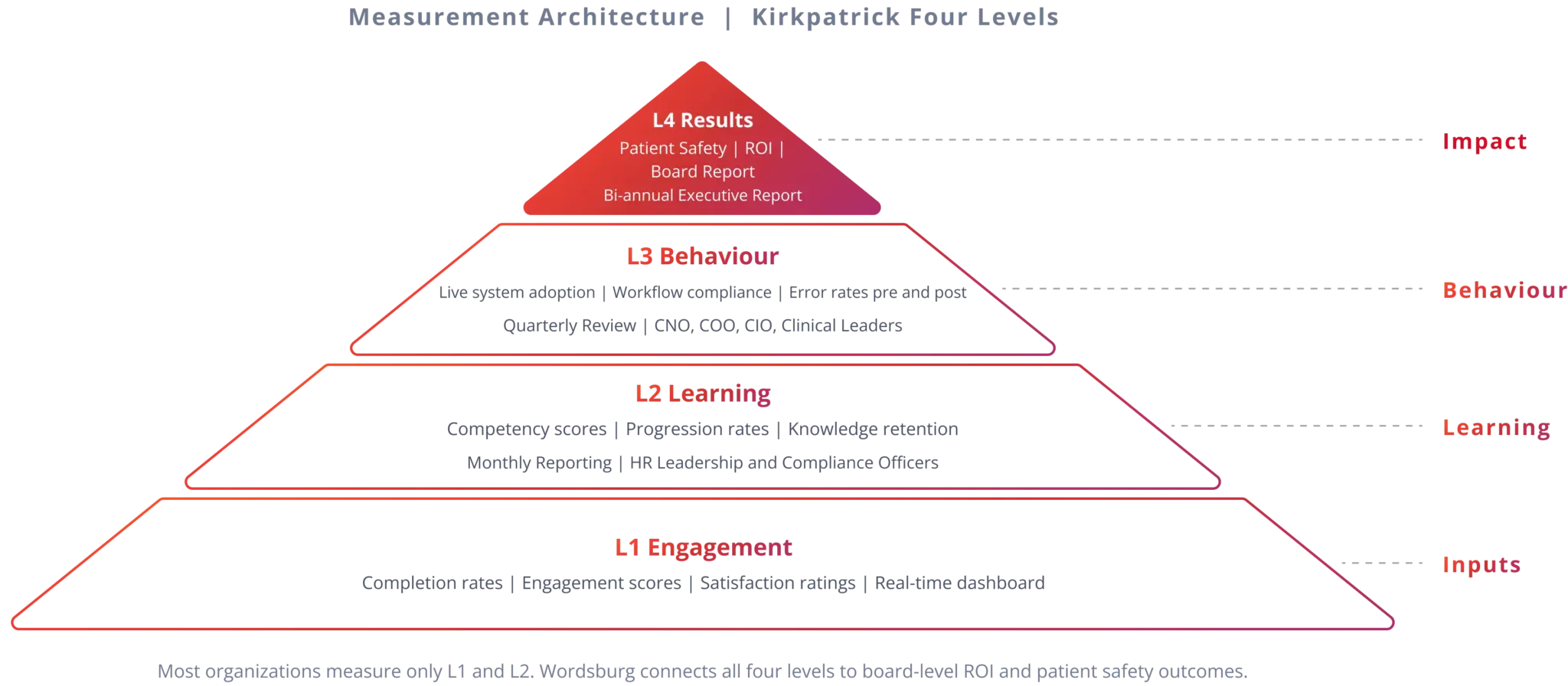
Kirkpatrick’s four-level measurement architecture is adapted for the healthcare digital transformation context.
| Level | Focus Question | Metrics Tracked | Reporting Cadence | Key Insight |
|---|---|---|---|---|
| L1 Engagement | Is the program reaching its audience? | – Completion rates – Engagement scores – Satisfaction ratings | Real-time via LMS dashboard | – Shows reach and engagement – Does not alone prove effectiveness |
| L2 Learning | Is learning actually happening? | – Competency scores – Progression rates – Knowledge retention | Monthly to HR and compliance | – Confirms staff can demonstrate required knowledge – Meets minimum regulatory reporting standard |
| L3 Behaviour | Are staff applying learning on the job? | – System adoption rates – Workflow compliance – Error frequency (before vs after) | Quarterly with key leaders | – Most programs struggle here – Transfer to daily operations is rarely supported or measured |
| L4 Results | What is the strategic and financial impact? | – Patient safety – Productivity – Compliance audit scores – ROI | Twice a year to leadership | – Links workforce investment to strategic results – Positions the CHRO as a strategic partner |
The Accountability Shift
Organizations that measure behaviour change and business results (Levels 3 and 4), not just completion rates, are far more likely to secure ongoing investment. They can show financial returns that matter to executives, and the data proves the program pays for itself.

Five Actions Healthcare Leaders Should Take Now
The window for proactive action on digital workforce readiness is narrowing. Regulatory pressure around AI governance is increasing. Vendor contracts for EHR and digital health platforms are tightening performance expectations. The organizations that invest in workforce readiness ahead of the curve will realize the full value of their digital infrastructure.

Five priority actions mapped by urgency, ownership, and strategic rationale for healthcare executive teams.
Digital transformation fails when people aren’t ready. Use this checklist to guide your organization’s effective digital transformation and workforce readiness.
Digital Skills Transformation Checklist
| ✓ | Action Items | Notes / Owner |
|---|---|---|
| Conduct A Digital Skills Audit | ||
| Assess skills across clinical, administrative, IT, and leadership teams | ||
| Map current skills to technology needs | ||
| Identify major gaps and risks | ||
| Establish a baseline for future investments | ||
| Prioritize Leadership Digital Fluency | ||
| Launch a structured digital fluency program for leaders | ||
| Begin at least 12 weeks before major technology deployment | ||
| Ensure leaders can assess AI, interpret data, and govern technology use | ||
| Tailor Training For Clinical Realities | ||
| Design training to fit real work patterns (short, flexible modules) | ||
| Avoid long, disruptive training sessions | ||
| Match training format, duration, and scheduling to audience needs | ||
| Dedicate 15-20% Of Tech Budgets To Training | ||
| Allocate 15–20% of project budgets for training and change management | ||
| Monitor spending to meet this benchmark | ||
| Build Outcome Measurement Frameworks | ||
| Set up systems to measure learning outcomes and business impact | ||
| Track behavioural changes, error rates, productivity recovery, and ROI |
Conclusion: The Human Edge In Digital Healthcare
Every healthcare system in the world is navigating the same tension: technology is advancing faster than the people charged with using it can keep up with. That gap is not permanent. It is a training problem with a training solution, but only if that solution is designed with the sophistication that healthcare’s operational complexity demands.
Purchasing an EHR without a workforce readiness program is the equivalent of installing the most advanced surgical equipment in a hospital with no surgeons trained to use it. The Wordsburg Digital Readiness Framework exists to close that gap, systematically, measurably, and at scale.
“The digital transformation of healthcare will not be completed by technologists. It will be completed by clinicians, administrators, and leaders who are equipped to use technology in the service of better human outcomes.”
